My my, sebastiantombs, aren't we cynical today?
")
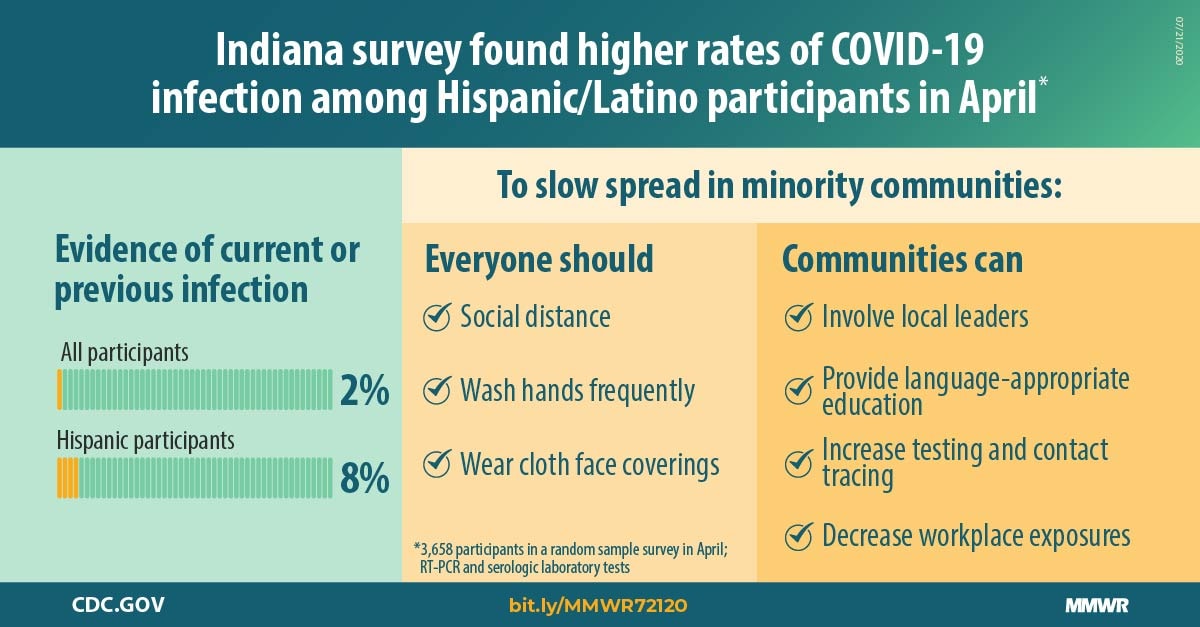
Actually guys, this is something that is important to study and various initiatives are doing just that. Here is one of them, based in Indiana, which I've posted here before but will refresh your memories and highlight it for those that didn't see it before:
In partnership with ISDH and the governor's office, the IU Richard M. Fairbanks School of Public Health has launched a year-long study of COVID-19 in Indiana.

fsph.iupui.edu
The initiative will collect data on active infections of randomly selected participants via PCR (which notably often remains positive for a week or more after being actively infectious) as well as data on past infection via antibody tests (which are getting better over time).
The study was designed to work in four waves. Data is available for the first wave, with sampling dates in late April, at the height of the first wave. You can dig through the data and reports, but here's the TL/DR for you. Based on the random sampling, in late April just shy of 3% of the Indiana population age >12 were considered to have had had COVID-19 infections, which was about
10x the number of documented cases in the state at that time. Of these infections, about 44% were asymptomatic. Overall IFR (infection death rate) of about 0.6%, which is ~6 times seasonal flu IFR for the whole population. Hopefully the next wave of data will be available soon; I think they did sampling again over the summer. Other studies I've heard of were in this 10x infections-to-cases ballpark.
OK, so, early on, when testing was hard to come by, 10X as many people had had infections as were documented as cases. So, you can use that as a high water mark. Tests are much easier to come by now (though, getting results in a useful time frame still often eludes us...) so it makes sense that as testing became more available, the ratio of infections to cases would have come down significantly, since pretty much anyone who gets a sniffle now is tested before they can return to work/school etc.. Of course since >40% of infections are asymptomatic, a lot of these people won't have reason to get tested. So the current minimum ratio between infections and cases is probably no lower than 6x. Let's split the difference and say as a rule of thumb, since the beginning of this thing, there have been 8x as many infections as cases.
Total cases in the US, per Worldometers today, is just shy of 6.6M. So, using our 8x multiplier, that suggests a ballpark of 53M Americans who had infections out of 331M.
About 16%. Disagree with my figures or assumptions? How about a window "more than 10%, less than 20%" of Americans have been infected. For sure, the reality is somewhere in there.
Let's just say "less than 20%" for purposes of discussion. This is way too low to offer any significant herd immunity, but some sectors will break that trend: groups that were hard hit early on now have a fair amount of people with some degree of immunity working there... Critical point:
meatpacking is working at good capacity and the bacon supply is plentiful. Repeat: bacon is plentiful.
However, natural immunity from coronavirus infections is believed to be fleeting. Sure, for a few months you're good. And after that you might get a less severe case due to lingering antibody protection, as long as you don't have a major risk factor going on (old, fat, cancer, heart disease). But this natural immunity tends to be much less powerful than vaccine-derived protection.
So we have been going on with this disease for 8 months and have less than a fifth of us infected. And the earliest infection are likely much less immune now than they were months ago... they could get it again, or at least will be vulnerable again soon enough. So Jessie is right, the virus is still there.
But getting infected isn't inevitable by any means. Mask up, minimize gatherings, work appropriately --like we're doing in Indiana for the most part--, minimize school density, and we can make it another 3-6 months to a vaccine. The only way we get to the other side is the vaccine. There are a bunch of them in the works, some using new technology and some with more tried and true methods, and I'm confident one or more of them will be ready for deployment in Q1 2021.
Recovered: As of today, 3.8M out of the 6.6M cases. Recovered is hard to measure as it's not always tracked, unlike deaths. However, something like 5-10% of COVID cases (cases, not infections) lead to lasting damage and problems (lung issues, clotting, heart issues). This is the great unremarked thing that's going on now. Lots of my doctor friends are strongly concerned about whether these impacts will be just for months, or permanent.