
Pandemic threat? Anyone else concerned?
- Thread starter erkme73
- Start date
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.

bigredfish
Known around here
Where is that data from?
I need to dig a bit deeper but that sounds counter opposite to published data from UK, Aus, Canada and others..
Of course there’s the whole cause of death thing that was recently shown to be over counted for Covid by 50-80%, so if we can’t believe the death count/cause of death, it makes it hard to believe this…
Oh and kids up to teens have had next to 0 deaths relative to the total…. Hmmmm
Fun with numbers…
I need to dig a bit deeper but that sounds counter opposite to published data from UK, Aus, Canada and others..
Of course there’s the whole cause of death thing that was recently shown to be over counted for Covid by 50-80%, so if we can’t believe the death count/cause of death, it makes it hard to believe this…
Oh and kids up to teens have had next to 0 deaths relative to the total…. Hmmmm
Fun with numbers…

Where is that data from?
I need to dig a bit deeper but that sounds counter opposite to published data from UK, Aus, Canada and others..
Of course there’s the whole cause of death thing that was recently shown to be over counted for Covid by 50-80%, so if we can’t believe the death count/cause of death, it makes it hard to believe this…
Oh and kids up to teens have had next to 0 deaths relative to the total…. Hmmmm
Fun with numbers…
CDC Data and here is the source. My comments are my interpretation and not the author's. The author is a Physician, Scientist, and the head of the Scripps Institute if I recall correctly. He is very pro vaccine and pro booster and obviously very smart but I do not agree with his stance on vaccines.

bigredfish
Known around here
Thx
Yeah I don’t believe CDC data. It runs counter to many others…
Yeah I don’t believe CDC data. It runs counter to many others…
bigredfish
Known around here
And as if to say “thanks for calling that out Bigredfish”, see this new article. Read down especially towards the bottom (with citations)
The excerpts I post below aren’t even 1/2 of the incredibly well documented and cited article. Highly recommend for anyone who wants to be up to date on where things stand.
The CDC data is at best tainted and more likely manipulated. (Or that Dr is taking his own liberties)
Why Is There A COVID Vaccine Mandate For Students?
 www.zerohedge.com
www.zerohedge.com
A Cleveland Clinic study of the bivalent vaccines involving 51,011 participants found the risk of getting COVID-19 increased “with the number of vaccine doses previously received”—much to the authors’ surprise.
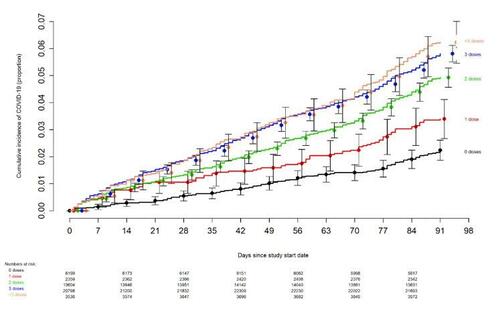
They were stumped as to why “those who chose not to follow the CDC’s recommendations on remaining updated with COVID-19 vaccination” had a lower risk of catching COVID than “those who received a larger number of prior vaccine doses.”
So if the vaccines don’t keep you from getting COVID, maybe they at least protect you from hospitalization?
That doesn’t wash, either, because according to data from the Coronavirus Disease 2019 (COVID-19)-Associated Hospitalization Surveillance Network (COVID-NET), hospitalization rates for 18–64-year-olds have increased 11 percent since the vaccine rollout. Worse, kids under 18 have suffered a shocking 74 percent spike in hospitalizations.
An observational study conducted at Germany’s University Hospital Wuerzburg found:
“The rate of adverse reactions for the second booster dose was significantly higher among participants receiving the bivalent 84.6% (95% CI 70.3%–92.8%; 33/39) compared to the monovalent 51.4% (95% CI 35.9–66.6%; 19/37) vaccine (p=0.0028). Also, there was a trend towards an increased rate of inability to work and intake of PRN medication following bivalent vaccination.”
A new paper published in Science titled Class Switch Towards Non-Inflammatory, Spike-Specific IgG4 Antibodies after Repeated SARS-CoV-2 mRNA Vaccination even has Eric Topol concerned: (<<<< Same Guy as quoted on the Tweet 2 posts up about how the Jab is effective)
If you don’t know what that means, Dr. Syed Haider spells it out in this tweet. He explains that the shots “train your immune system to ignore the allergen by repeated exposure,” the end result being that “Your immune system is shifted to see the virus as a harmless allergen” and the “virus runs amok.”
Viral immunologist and computational virologist Dr. Jessica Rose breaks down the serious implications—including cancer, fatal fibrosis, and organ destruction—of these findings.
Well, then does the vaccine at least prevent people from dying of COVID?
Nope. According to the Washington Post, “Vaccinated people now make up a majority of COVID deaths.”
At Senator Ron Johnson’s December 7, 2022, roundtable discussion on COVID-19 Vaccines, former number-one–ranked Wall Street insurance analyst Josh Stirling reported that, according to UK government data:
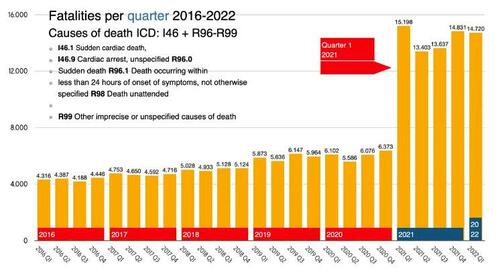
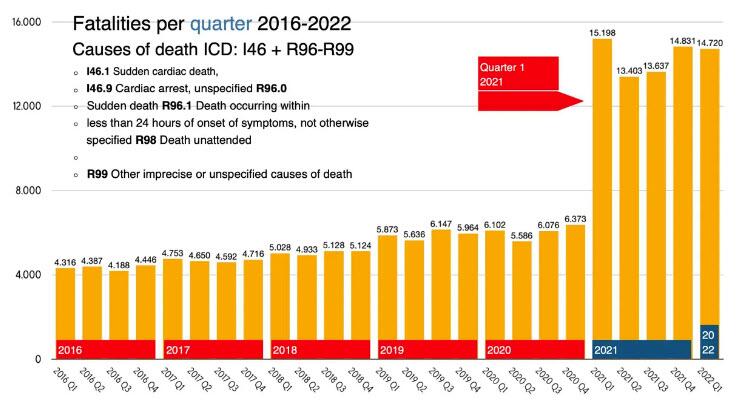
Data analyst Tom Lausen assessed the ICD-10 disease codes in this dataset, and the findings are startling. His presentation includes the following chart documenting fatalities per quarter from 2016 to 2022:
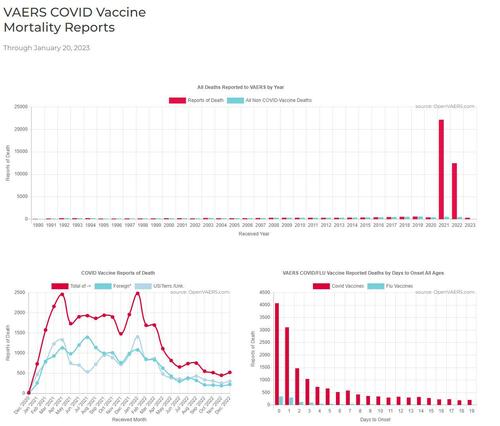
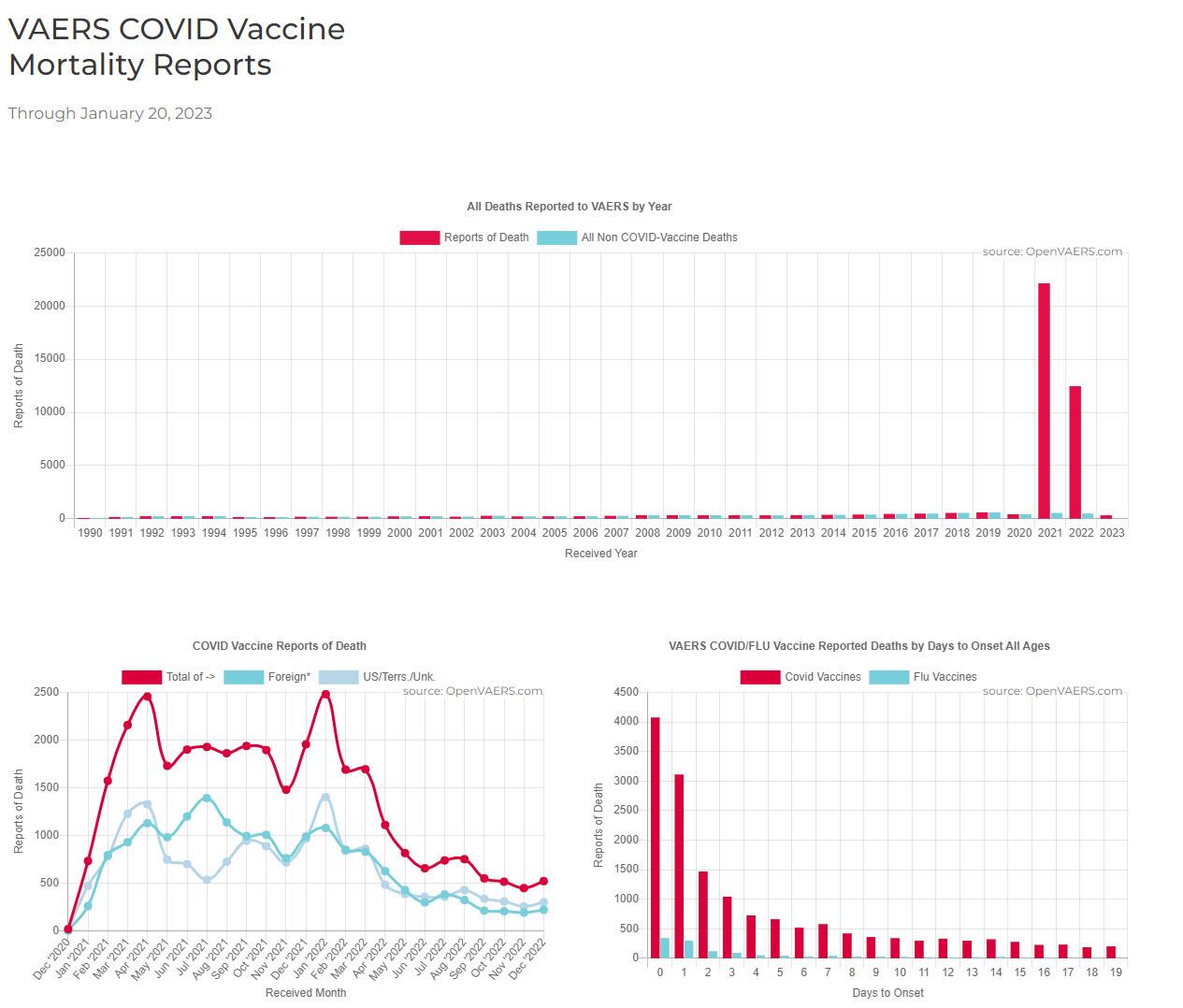
This parallels the skyrocketing fatality rates seen in VAERS:
The vaccinated are more likely to contract, become hospitalized from, and die of COVID. If the vaccine fails on all of those counts, does it at least prevent its transmission to other students and community members?
The obvious answer is no since we already know it doesn’t prevent you from getting COVID, but this CDC study drives the point home, showing that during a COVID outbreak in Barnstable County, Massachusetts, “three quarters (346; 74%) of cases occurred in fully vaccinated persons.”
Maybe Stanford can tell us why they feel the mandate is necessary. Their booster requirement reads:
Speaking of not keeping up, that same article says the new bivalent boosters target “the original version of the coronavirus and the Omicron variants circulating earlier this year, BA.4 and BA.5.”
It then goes on to quote Head of Beth Israel Deaconess’s Center for Virology & Vaccine Research Dan Barouch, who says, “It’s not likely that any of the vaccines or boosters, no matter how many you get, will provide substantial and sustained protection against acquisition of infection.”
In other words, Stanford’s rationale for requiring the boosters is obsolete according to the authority they cite in their justification.
If Stanford is genuinely concerned about “reduc[ing] the possibility of widespread disruptions that could impact the student experience,” then it should not only stop mandating the vaccine but advise against it.
Some nations have suspended or recommended against COVID shots for younger populations due to the considerable risks of adverse events such as pulmonary embolism and myocarditis—from Denmark (under 50) to Norway (under 45) to Australia (under 50) to the United Kingdom (seasonal boosters for under 50).
The Danish Health Authority explains why people under 50 are “not to be re-vaccinated”:
This mirrors my own findings that myocarditis rates are up 10 times among the vaccinated according to a public healthcare worker survey.
Coauthored by MIT professor and risk management expert Retsef Levi, the Nature article Increased Emergency Cardiovascular Events Among Under-40 Population in Israel During Vaccine Rollout and Third COVID-19 Wave reveals a 25 percent increase in cardiac emergency calls for 16–39-year-olds from January to May 2021 as compared with the previous two years.
The paper cites a study by Israel’s Ministry of Health that “assesses the risk of myocarditis after receiving the 2nd vaccine dose to be between 1 in 3000 to 1 in 6000 in men of age 16–24 and 1 in 120,000 in men under 30.”
A Thai study published in Tropical Medicine and Infectious Disease found cardiovascular manifestations in 29.24 percent of the adolescent cohort—including myopericarditis and tachycardia.
Even Dr. Leana Wen, formerly an aggressive promoter of the COVID vaccine, admitted in a recent Washington Post op-ed:
Formerly pro-vaxx cardiologists such as Dr. Aseem Malhotra, Dr. Dean Patterson, and Dr. Ross Walker are all saying the COVID vaccines should be immediately stopped due to the significant increase in cardiac diseases, adverse events, and excess mortality observed since their rollout, noting that, “until proven otherwise, these vaccines are not safe.”
——
According to British Medical Journal Senior Editor Dr. Peter Doshi, Pfizer’s and Moderna’s own trial data found 1 in 800 vaccinated people experienced serious adverse events:
And this is the same Pfizer data the FDA tried to keep hidden from the public for 75 years.
Nothing to see here … except 1,223 deaths, 158,000 adverse events, and 1,291 side effects reported in the first 90 days according to the 5.3.6 Cumulative Analysis of Post-Authorization Adverse Event Reports—and those numbers are likely underreported by a factor of at least 10 (my conservative calculations show an underreporting factor (URF) of 41 for VAERS)
Let’s recap.
Abundant evidence proves the vaccines FAIL to:
LOTS More Here:
www.zerohedge.com
The excerpts I post below aren’t even 1/2 of the incredibly well documented and cited article. Highly recommend for anyone who wants to be up to date on where things stand.
The CDC data is at best tainted and more likely manipulated. (Or that Dr is taking his own liberties)
Why Is There A COVID Vaccine Mandate For Students?
ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
A Cleveland Clinic study of the bivalent vaccines involving 51,011 participants found the risk of getting COVID-19 increased “with the number of vaccine doses previously received”—much to the authors’ surprise.

They were stumped as to why “those who chose not to follow the CDC’s recommendations on remaining updated with COVID-19 vaccination” had a lower risk of catching COVID than “those who received a larger number of prior vaccine doses.”
So if the vaccines don’t keep you from getting COVID, maybe they at least protect you from hospitalization?
That doesn’t wash, either, because according to data from the Coronavirus Disease 2019 (COVID-19)-Associated Hospitalization Surveillance Network (COVID-NET), hospitalization rates for 18–64-year-olds have increased 11 percent since the vaccine rollout. Worse, kids under 18 have suffered a shocking 74 percent spike in hospitalizations.
An observational study conducted at Germany’s University Hospital Wuerzburg found:
“The rate of adverse reactions for the second booster dose was significantly higher among participants receiving the bivalent 84.6% (95% CI 70.3%–92.8%; 33/39) compared to the monovalent 51.4% (95% CI 35.9–66.6%; 19/37) vaccine (p=0.0028). Also, there was a trend towards an increased rate of inability to work and intake of PRN medication following bivalent vaccination.”
A new paper published in Science titled Class Switch Towards Non-Inflammatory, Spike-Specific IgG4 Antibodies after Repeated SARS-CoV-2 mRNA Vaccination even has Eric Topol concerned: (<<<< Same Guy as quoted on the Tweet 2 posts up about how the Jab is effective)
If you don’t know what that means, Dr. Syed Haider spells it out in this tweet. He explains that the shots “train your immune system to ignore the allergen by repeated exposure,” the end result being that “Your immune system is shifted to see the virus as a harmless allergen” and the “virus runs amok.”
Viral immunologist and computational virologist Dr. Jessica Rose breaks down the serious implications—including cancer, fatal fibrosis, and organ destruction—of these findings.
Well, then does the vaccine at least prevent people from dying of COVID?
Nope. According to the Washington Post, “Vaccinated people now make up a majority of COVID deaths.”
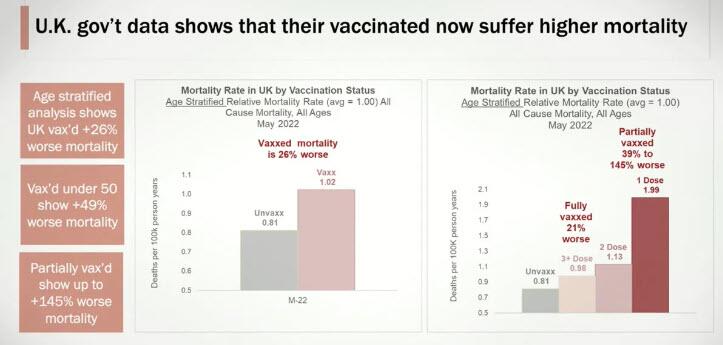
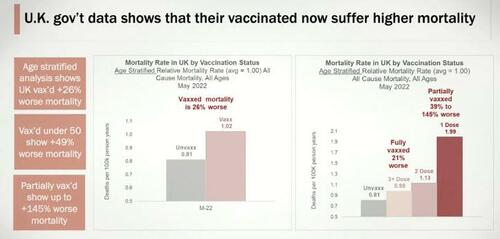
At Senator Ron Johnson’s December 7, 2022, roundtable discussion on COVID-19 Vaccines, former number-one–ranked Wall Street insurance analyst Josh Stirling reported that, according to UK government data:
Obtained by a Freedom of Information Act (FOIA) request to KBV (the association representing physicians who receive insurance in Germany), “the most important dataset of the pandemic” shows fatalities starting to spike in 2021.“The people in the UK who took the vaccine have a 26% higher mortality rate. The people who are under the age of 50 who took the vaccine now have a 49% higher mortality rate.”
Data analyst Tom Lausen assessed the ICD-10 disease codes in this dataset, and the findings are startling. His presentation includes the following chart documenting fatalities per quarter from 2016 to 2022:
This parallels the skyrocketing fatality rates seen in VAERS:
The vaccinated are more likely to contract, become hospitalized from, and die of COVID. If the vaccine fails on all of those counts, does it at least prevent its transmission to other students and community members?
The obvious answer is no since we already know it doesn’t prevent you from getting COVID, but this CDC study drives the point home, showing that during a COVID outbreak in Barnstable County, Massachusetts, “three quarters (346; 74%) of cases occurred in fully vaccinated persons.”
Maybe Stanford can tell us why they feel the mandate is necessary. Their booster requirement reads:
The claim that “booster shots enhance immunity” links to a January 2022 New York Times article. It seems Stanford has failed to keep up with the science because the very source they cite as authoritative is now reporting, “The newer variants, called BQ.1 and BQ.1.1, are spreading quickly, and boosters seem to do little to prevent infections with these viruses.”“Why does Stanford have a student booster shot requirement? Our booster requirement is intended to support sustained immunity against COVID-19 and is consistent with the advice of county and federal public health leaders. Booster shots enhance immunity, providing additional protection to individuals and reducing the possibility of being hospitalized for COVID. In addition, booster shots prevent infection in many individuals, thereby slowing the spread of the virus. A heavily boosted campus community reduces the possibility of widespread disruptions that could impact the student experience, especially in terms of in-person classes and activities and congregate housing.”
Speaking of not keeping up, that same article says the new bivalent boosters target “the original version of the coronavirus and the Omicron variants circulating earlier this year, BA.4 and BA.5.”
It then goes on to quote Head of Beth Israel Deaconess’s Center for Virology & Vaccine Research Dan Barouch, who says, “It’s not likely that any of the vaccines or boosters, no matter how many you get, will provide substantial and sustained protection against acquisition of infection.”
In other words, Stanford’s rationale for requiring the boosters is obsolete according to the authority they cite in their justification.
If Stanford is genuinely concerned about “reduc[ing] the possibility of widespread disruptions that could impact the student experience,” then it should not only stop mandating the vaccine but advise against it.
Some nations have suspended or recommended against COVID shots for younger populations due to the considerable risks of adverse events such as pulmonary embolism and myocarditis—from Denmark (under 50) to Norway (under 45) to Australia (under 50) to the United Kingdom (seasonal boosters for under 50).
The Danish Health Authority explains why people under 50 are “not to be re-vaccinated”:
Here’s what a Norwegian physician and health official had to say:“People aged under 50 are generally not at particularly higher risk of becoming severely ill from covid-19. In addition, younger people aged under 50 are well protected against becoming severely ill from covid-19, as a very large number of them have already been vaccinated and have previously been infected with covid-19, and there is consequently good immunity among this part of the population.”
“Especially the youngest should consider potential side effects against the benefits of taking this dose.”
—Ingrid Bjerring, Chief Doctor at Lier Municipality
A new Nordic cohort study of 8.9 million participants supports these concerns, finding a nearly nine-fold increase in myocarditis among males aged 12–39 within 28 days of receiving the Moderna COVID-19 booster over those who stopped after two doses.“We did not find sufficient evidence to recommend that this part of the population [younger age bracket] should take a new dose now.… Each vaccine comes with the risk for side effects. Is it then responsible to offer this, when we know that the individual health benefit of a booster likely is low?”
—Are Stuwitz Berg, Department Director at the Norwegian Institute of Public Health
This mirrors my own findings that myocarditis rates are up 10 times among the vaccinated according to a public healthcare worker survey.
Coauthored by MIT professor and risk management expert Retsef Levi, the Nature article Increased Emergency Cardiovascular Events Among Under-40 Population in Israel During Vaccine Rollout and Third COVID-19 Wave reveals a 25 percent increase in cardiac emergency calls for 16–39-year-olds from January to May 2021 as compared with the previous two years.
The paper cites a study by Israel’s Ministry of Health that “assesses the risk of myocarditis after receiving the 2nd vaccine dose to be between 1 in 3000 to 1 in 6000 in men of age 16–24 and 1 in 120,000 in men under 30.”
A Thai study published in Tropical Medicine and Infectious Disease found cardiovascular manifestations in 29.24 percent of the adolescent cohort—including myopericarditis and tachycardia.
Even Dr. Leana Wen, formerly an aggressive promoter of the COVID vaccine, admitted in a recent Washington Post op-ed:
All over the world, prominent physicians, scientists, politicians, and professors are asking pointed questions about illogical mandates; the safety and efficacy of the vaccines; and the dangers posed by the mRNA technology, spike protein, and lipid nanoparticles—including in the UK, Japan, Australia, Europe, and the US.“[W]e need to be upfront that nearly every intervention has some risk, and the coronavirus vaccine is no different. The most significant risk is myocarditis, an inflammation of the heart muscle, which is most common in young men. The CDC cites a rate of 39 myocarditis cases per 1 million second doses given in males 18 to 24. Some studies found a much higher rate; a large Canadian database reported that among men ages 18 to 29 who received the second dose of the Moderna vaccine, the rate of myocarditis was 22 for every 100,000 doses.”
Formerly pro-vaxx cardiologists such as Dr. Aseem Malhotra, Dr. Dean Patterson, and Dr. Ross Walker are all saying the COVID vaccines should be immediately stopped due to the significant increase in cardiac diseases, adverse events, and excess mortality observed since their rollout, noting that, “until proven otherwise, these vaccines are not safe.”
——
According to British Medical Journal Senior Editor Dr. Peter Doshi, Pfizer’s and Moderna’s own trial data found 1 in 800 vaccinated people experienced serious adverse events:
And this is the same Pfizer data the FDA tried to keep hidden from the public for 75 years.
Nothing to see here … except 1,223 deaths, 158,000 adverse events, and 1,291 side effects reported in the first 90 days according to the 5.3.6 Cumulative Analysis of Post-Authorization Adverse Event Reports—and those numbers are likely underreported by a factor of at least 10 (my conservative calculations show an underreporting factor (URF) of 41 for VAERS)
Let’s recap.
Abundant evidence proves the vaccines FAIL to:
- stop transmission
- prevent contraction of COVID
- lower hospitalization rates
- reduce mortality
- heightened transmission levels
- greater chances of catching COVID
- increased hospitalization rates
- higher excess mortality
- disproportionate injuries to women
LOTS More Here:
ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
Last edited:
As an Amazon Associate IPCamTalk earns from qualifying purchases.
mat200
IPCT Contributor
- Jan 17, 2017
- 19,182
- 32,097
Summary: Delta was bad .. Omicron less so .. Risk has changed ..
UK data, massive shift in vaccine risk / benefit analysis
UK data, massive shift in vaccine risk / benefit analysis

Massive meta-study on mask wearing delivers kill shot to COVID narrative * WorldNetDaily * by Peter LaBarbera
Wearing face-masks — even fancier N95 masks — has "little or no" effect in protecting against COVID-19 and the flu compared to not wearing one, according to a massive new British meta-study.
 www.wnd.com
www.wnd.com
bigredfish
Known around here

Ssayer
BIT Beta Team

Oceanslider
Known around here


bigredfish
Known around here
Recent Data Shows 'Stunning Increase' In Serious Harm Reports In Young Healthy Pilots: Army Lt. Col. Theresa Long
www.zerohedge.com
That’s according to Lt. Col.Theresa Long, M.D., MPH, a board-certified aerospace medicine doctor and Army Brigade flight surgeon with specialty training as an aviation mishap investigator and safety officer, who was one of the four whistleblowers. Long’s background has uniquely equipped her to recognize what she described as “unusual diagnoses and alarming trends only after the introduction of the COVID-19 vaccinations.”
Sharp Increase in Serious Harm Reports in Pilots: DOD Data
Long said what she has now found has led her to file yet another whistleblower complaint with Sen. Ron Johnson’s (R-Wis.) office. She described this data as “more alarming DMED data” after she “went back into the ‘fixed’ DMED again to look for signals of harm for Army aviation.”
“What I found was a clear signal, that something in 2021 changed the health of service members,” Long told The Epoch Times. She said these signals were consistent with those in the Vaccine Adverse Event Reporting System (VAERS) reports. But unlike VAERS reports, DMED data showed spikes in the number of diagnoses “made by a healthcare professional within the DOD on service members.”
According to the Military Health System, the DMED provides remote access to a subset of data contained in the Defense Medical Surveillance System (DMSS). The DMSS contains up-to-date and historical data on diseases and medical events (including reportable events) and “is available to authorized users such as U.S. military medical providers, epidemiologists, medical researchers, safety officers or medical operations/ clinical support staff for surveying health conditions in the U.S. military.”
“After querying all pilots across the DOD, for all-cause morbidity and mortality, I found a stunning increase in the number of reportable events, spiking from an average of 226 reportable events a year (2016-2019) to 4,059 reports in 2022,” she explained.
A DOD reportable event is any patient safety event resulting in death, permanent harm, or severe temporary harm—and all require a comprehensive systematic analysis and a follow-on corrective action implementation plan report.
ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
www.zerohedge.com
That’s according to Lt. Col.Theresa Long, M.D., MPH, a board-certified aerospace medicine doctor and Army Brigade flight surgeon with specialty training as an aviation mishap investigator and safety officer, who was one of the four whistleblowers. Long’s background has uniquely equipped her to recognize what she described as “unusual diagnoses and alarming trends only after the introduction of the COVID-19 vaccinations.”
Sharp Increase in Serious Harm Reports in Pilots: DOD Data
Long said what she has now found has led her to file yet another whistleblower complaint with Sen. Ron Johnson’s (R-Wis.) office. She described this data as “more alarming DMED data” after she “went back into the ‘fixed’ DMED again to look for signals of harm for Army aviation.”
“What I found was a clear signal, that something in 2021 changed the health of service members,” Long told The Epoch Times. She said these signals were consistent with those in the Vaccine Adverse Event Reporting System (VAERS) reports. But unlike VAERS reports, DMED data showed spikes in the number of diagnoses “made by a healthcare professional within the DOD on service members.”
According to the Military Health System, the DMED provides remote access to a subset of data contained in the Defense Medical Surveillance System (DMSS). The DMSS contains up-to-date and historical data on diseases and medical events (including reportable events) and “is available to authorized users such as U.S. military medical providers, epidemiologists, medical researchers, safety officers or medical operations/ clinical support staff for surveying health conditions in the U.S. military.”
“After querying all pilots across the DOD, for all-cause morbidity and mortality, I found a stunning increase in the number of reportable events, spiking from an average of 226 reportable events a year (2016-2019) to 4,059 reports in 2022,” she explained.
A DOD reportable event is any patient safety event resulting in death, permanent harm, or severe temporary harm—and all require a comprehensive systematic analysis and a follow-on corrective action implementation plan report.


VorlonFrog
Known around here
Excerpt of video with Dr. Drew Pinsky

 rumble.com
rumble.com
Dr. Ryan Cole Shares Terrifying Biopsy Results Which Could Explain Rise in Cancers
“All that blue — those are cancer cells. What’s inside of every cancer cell? Spike protein. Every B-cell there that’s malignant has spike protein in it.”
rumble.com
Ssayer
BIT Beta Team
Presuming this is what it appears to be at face value, might the egg shortage make more sense now?

 www.sciencedirect.com
www.sciencedirect.com
Chicken Egg Yolk Antibodies (IgYs) block the binding of multiple SARS-CoV-2 spike protein variants to human ACE2
The SARS-CoV-2 virus is still spreading worldwide, and there is an urgent need to effectively prevent and control this pandemic. This study evaluated …
www.sciencedirect.com
Egg prices have gotten so high that my favorite breakfast place (called The Breakfast Place) is talking about closing down. They are currently loosing money and have already raised prices back in November(?) I think it was. They got a lot of flak about raising the prices but I thought they were still very reasonable. I hope they can hold on until the prices come back down.
Ssayer
BIT Beta Team
Their prices will go down about the same time taxes go down (can you say never? I thought you could)
Prices simply will NOT be going down in USD...
Prices simply will NOT be going down in USD...
Ssayer
BIT Beta Team


Recent Data Shows 'Stunning Increase' In Serious Harm Reports In Young Healthy Pilots: Army Lt. Col. Theresa Long
ZeroHedge
ZeroHedge - On a long enough timeline, the survival rate for everyone drops to zero
That’s according to Lt. Col.Theresa Long, M.D., MPH, a board-certified aerospace medicine doctor and Army Brigade flight surgeon with specialty training as an aviation mishap investigator and safety officer, who was one of the four whistleblowers. Long’s background has uniquely equipped her to recognize what she described as “unusual diagnoses and alarming trends only after the introduction of the COVID-19 vaccinations.”
Sharp Increase in Serious Harm Reports in Pilots: DOD Data
Long said what she has now found has led her to file yet another whistleblower complaint with Sen. Ron Johnson’s (R-Wis.) office. She described this data as “more alarming DMED data” after she “went back into the ‘fixed’ DMED again to look for signals of harm for Army aviation.”
“What I found was a clear signal, that something in 2021 changed the health of service members,” Long told The Epoch Times. She said these signals were consistent with those in the Vaccine Adverse Event Reporting System (VAERS) reports. But unlike VAERS reports, DMED data showed spikes in the number of diagnoses “made by a healthcare professional within the DOD on service members.”
According to the Military Health System, the DMED provides remote access to a subset of data contained in the Defense Medical Surveillance System (DMSS). The DMSS contains up-to-date and historical data on diseases and medical events (including reportable events) and “is available to authorized users such as U.S. military medical providers, epidemiologists, medical researchers, safety officers or medical operations/ clinical support staff for surveying health conditions in the U.S. military.”
“After querying all pilots across the DOD, for all-cause morbidity and mortality, I found a stunning increase in the number of reportable events, spiking from an average of 226 reportable events a year (2016-2019) to 4,059 reports in 2022,” she explained.
A DOD reportable event is any patient safety event resulting in death, permanent harm, or severe temporary harm—and all require a comprehensive systematic analysis and a follow-on corrective action implementation plan report.
Why Are the EKGs of Pilots No Longer Normal?
STORY AT-A-GLANCE
- Oct. 24, 2022, the FAA changed the EKG requirements necessary for pilots to fly—but not to make them safer.
- With no public announcement or explanation, the agency expanded the allowable range for PR, a measure of heart function.
- Widening this parameter means those with potential heart damage are now allowed to fly commercial aircraft, potentially putting passengers at risk, should they suffer a heart attack or other event while in the air.
- Evidence suggests that pilots’ worsening heart health is due to adverse effects of COVID-19 shots.
- An estimated 20 percent of pilots screened may have suffered heart damage due to COVID-19 shots, and the FAA may have been forced to widen the EKG parameters so pilots could continue to fly.
Oct. 24, 2022, the FAA changed the EKG requirements necessary for pilots to fly—but not to make them safer. With no public announcement or explanation, the agency expanded the allowable range for the PR interval, a measure of heart function.2
Widening this parameter means those with potential heart damage, disease, or injuries are now allowed to fly commercial aircraft, potentially putting passengers at risk, should they suffer a heart attack or other event while in the air. Why would the FAA make such a drastic and risky move without informing the public?
COVID SHOTS MAY HAVE DAMAGED PILOTS’ HEARTS
On an EKG, a normal PR interval measures 0.12 to 0.2 seconds.3 If the PR interval is shorter or longer than this, it can be indicative of a problem. According to Steve Kirsch, executive director of the Vaccine Safety Research Foundation, the FAA widened the acceptable EKG parameters from a PR max of 0.2 to 0.3, and potentially even higher. He says:4
Kirsch gives five reasons why he’s confident these widened parameters were necessary due to the widespread heart damage pilots—and the U.S. public—experienced due to COVID-19 shots. According to Kirsch:5“They didn’t widen the range by a little. They widened it by a lot. It was done after the vaccine rollout. This is extraordinary. They did it hoping nobody would notice. It worked for a while. Nobody caught it. But you can’t hide these things for long. This is a tacit admission from the U.S. government that the COVID vaccine has damaged the hearts of our pilots. Not just a few pilots. A lot of pilots and a lot of damage.”
“I believe it is because they knew if they kept the original range, too many pilots would have to be grounded. That would be extremely problematic; commercial aviation in the U.S. would be severely disrupted. And why did they do that quietly without notifying the public or the mainstream media?
Story continues,“I’m pretty sure they won’t tell me, so I’ll speculate: it’s because they didn’t want anyone to know. In other words, the COVID vaccine has seriously injured a lot of pilots and the FAA knows it and said nothing because that would tip off the country that the vaccines are unsafe. And you aren’t allowed to do that.”
The Epoch Times | Breaking News, Latest News, World News and Videos
Get the latest breaking news, in-depth reporting, and insightful analysis on a wide range of topics, including politics, culture, and world events | The Epoch Times is a trusted source for real news and information that is free from influence and bias.
 www.theepochtimes.com
www.theepochtimes.com
Parley
Known around here
It's Time for the Scientific Community to Admit We Were Wrong About COVID and It Cost Lives | Opinion
As a medical student and researcher, I staunchly supported the efforts of the public health authorities when it came to COVID-19. I believed that the authorities responded to the largest public health crisis of our lives with compassion, diligence, and scientific expertise. I was with them when they called for lockdowns, vaccines, and boosters.
I was wrong. We in the scientific community were wrong. And it cost lives.
I can see now that the scientific community from the CDC to the WHO to the FDA and their representatives, repeatedly overstated the evidence and misled the public about its own views and policies, including on natural vs. artificial immunity, school closures and disease transmission, aerosol spread, mask mandates, and vaccine effectiveness and safety, especially among the young. All of these were scientific mistakes at the time, not in hindsight. Amazingly, some of these obfuscations continue to the present day.
My comment: From Newsweek no less.
As a medical student and researcher, I staunchly supported the efforts of the public health authorities when it came to COVID-19. I believed that the authorities responded to the largest public health crisis of our lives with compassion, diligence, and scientific expertise. I was with them when they called for lockdowns, vaccines, and boosters.
I was wrong. We in the scientific community were wrong. And it cost lives.
I can see now that the scientific community from the CDC to the WHO to the FDA and their representatives, repeatedly overstated the evidence and misled the public about its own views and policies, including on natural vs. artificial immunity, school closures and disease transmission, aerosol spread, mask mandates, and vaccine effectiveness and safety, especially among the young. All of these were scientific mistakes at the time, not in hindsight. Amazingly, some of these obfuscations continue to the present day.
My comment: From Newsweek no less.
bigredfish
Known around here
bigredfish
Known around here
Presuming this is what it appears to be at face value, might the egg shortage make more sense now?
Chicken Egg Yolk Antibodies (IgYs) block the binding of multiple SARS-CoV-2 spike protein variants to human ACE2
The SARS-CoV-2 virus is still spreading worldwide, and there is an urgent need to effectively prevent and control this pandemic. This study evaluated …
Thats actually damn interesting, and no I won’t jump to the conspiracy theory conclusion, …. Yet
")